|
Case Report
Vertebro-medullary hydatidosis: A case report
1 Radiology Resident, Medical Imaging Department, Faculty of Medicine and Pharmacy Mohammed V, Ibn Sina University Hospital Center, Street Lamfadel Cherkaoui, Rabat, Morocco
Address correspondence to:
Fabrice Diekouadio
Medical Imaging Department, Faculty of Medicine and Pharmacy Mohammed V, Ibn Sina University Hospital Center, Street Lamfadel Cherkaoui, Rabat 6527,
Morocco
Message to Corresponding Author
Article ID: 100016R02FD2020
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Diekouadio F, Semboung S, Boris B, El Bakkari A, Laamrani FZ. Vertebro-medullary hydatidosis: A case report. Edorium J Radiol 2020;6:100016R02FD2020.ABSTRACT
Echinococcosis is an endemic parasitic disease that affects mainly the liver and lungs. Exceptionally, there may be bone locations; the most common vertebro-medullary manifestation is bone hydatid disease. The evolution of this pathology is insidious; and the clinical manifestations are nonspecific. They are dominated by back pain and signs of spinal cord compression. We report the case of a 39-year-old patient, admitted for paraplegia, of progressive onset and insidious evolution over one year. Diagnosis was made with the aid of serology specific for hydatidosis, imaging, and confirmation on anatomopathology after surgical resection. The patient was put on albendazole after surgery.
Keywords: Cyst, Hydatidosis, Vertebro-medullary
INTRODUCTION
Hydatidosis is an anthropozoonosis caused by a parasite called Echinococcus granulosus. It mainly affects the liver and lungs, but can also affect other locations.
Vertebro-medullary hydatidosis remains rare, but represents the most serious form of bone damage in echinococcosis. We will report the case of a patient with vertebral-medullary hydatidosis, with extension to the ribs and para-vertebral soft parts.
CASE REPORT
H.A., aged 39, with no particular pathological history, was admitted to the Neurosurgery Department for a paraplegia that has progressed gradually for 1 year, with mechanical back pain, not improved by analgesics and anti-inflammatory drugs; without any notion of fever, nor of night sweat.
The clinical examination found paraplegia with abolition of the osteotendinous reflexes and deep and superficial sensitivity disorders. Biologically, the sedimentation rate is 32 mm in the first hour and the C-reactive protein (CRP) is 4 mg/L. The hydatid serology was positive.
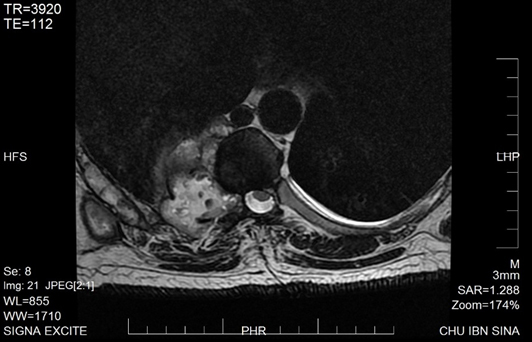
A magnetic resonance imaging (MRI) of the dorsolumbar spine was performed (G.E., 1.5 Tesla, triplanar acquisitions in T1, T2 weighted sequences without and with suppression of the fat signal, then injection of gadolinium), which demonstrated a liquid paravertebral lesional process, lateralized to the right, invading the vertebral bodies of D6 and D7, with T1 hypointense and heterogeneous T2 hypersignal.
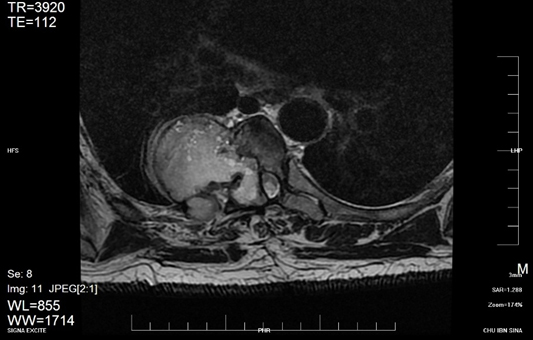
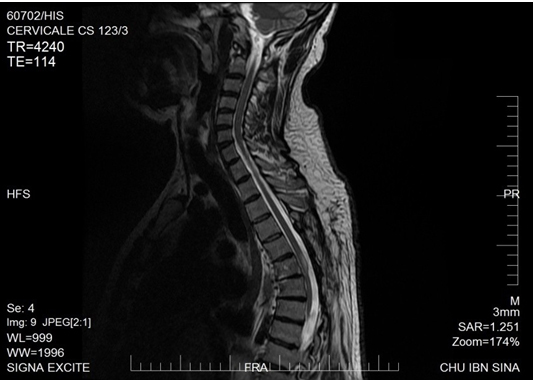
This process escapes through the inter-costal spaces to the right paravertebral soft parts where it organizes into a collection (Figure 1), infiltrates the vertebral bodies, the foramina, and also infiltrates the medullary canal, exerting a mass effect on the cord (Figure 2), which presents a hyper signal T2, reflecting a medullary distress (Figure 3). In addition, it lyses and invades the transverse processes of D7 and D8.
The results of the extension to search for other hydatid sites came back negative. The diagnosis was confirmed by histology after surgical removal of the process. The patient was put on albendazole.
DISCUSSION
Echinococcosis is an anthropozoonosis caused by Echinococcus granulosus, a dog tapeworm, in its larval form. The cycle of this parasite passes through intermediate hosts and definitive hosts. Intermediate hosts in the parasite’s cycle are herbivores, usually sheep, which explains the preponderance of this pathology in rural areas.
In the digestive tract of the intermediate host, the eggs release larvae that will lodge in the viscera through the blood. The organs most often affected are the liver and lungs. At this level, the larvae organize themselves into a hydatid cyst; the cycle will be completed after consumption of viscera infested by a definitive host (dog). The adult tapeworm then develops in the digestive tract of the definitive host and lays eggs which are passed in the stool. Humans represent an accidental host, through direct contact with the infested dog and ingestion of parasite eggs, and therefore constitute a parasitic impasse.
The bony localization of hydatid cyst is rare; and spinal hydatidosis is the most common and severe bone damage [1]. This is a rare localization, even in endemic countries.
Clinically, the course is insidious, with nonspecific clinical signs. The general condition remains long preserved; fever only occurs with superinfection. Pain is the earliest and most frequent symptom; local swelling of the soft tissue and pathological fractures can also occur. This development is rather slow, but inevitable toward medullary or radicular compression, by invasion of the medullary canal. Neurological involvement occurs gradually, leading to paraplegia in 25–50% of cases [2]. There may be a problem of differential diagnosis with infectious pathologies (tuberculous spondylodiscitis) or tumors (metastasis).
Hydatid serology is a test of choice for diagnosis, but it only becomes positive at the stage of soft tissue invasion or reworked cysts [3].
Standard X-rays help localize lesions and detect bone damage by the presence of lacunar images without peripheral sclerosis, of varying size and shape. Computed tomography (CT) makes it possible to better define bone lesions, to assess intracanal extension and therefore to better guide the surgical procedure.
Magnetic resonance imaging is the exam of choice for looking for signs of spinal cord compression. It makes it possible to detect signs of spinal cord suffering (Figure 3), to specify the relationship between hydatid vesicles and the dural sheath [4].
It also allows prolonged surveillance [5]. On MRI, hydatid vesicles, in their typical forms, appear in T1 hypointense and T2 hypersignal [6]. An enhancement of the walls or septa may be observed in the case of modified cysts [7].
At present, vertebral medullary hydatidosis presents a therapeutic difficulty, due to recurrences, and the partial or complete neurological deficit which may persist. The treatment of this pathology is mainly surgical. It consists of excising the lesions as widely as possible to avoid recurrence, which is frequent at this level [8].
Antihelminthic medical treatment based on azole derivatives serves as adjunct therapy to surgery, and is also indicated in inoperable forms [9].
CONCLUSION
Vertebro-medullary hydatidosis is rare, but serious, and has a poor prognosis due to its location. It is characterized by a slow but inevitable evolution toward medullary or radicular compression; hence the value of making an early diagnosis (CT, MRI) in order to improve the prognosis. The treatment is based on surgical excision, which must be complete, as recurrence is frequent.
REFERENCES
1.
Semlali S, Nassar I, Cissé A, El-Gueddari FZ, Imani F. Cervical hydatid disease with retropharyngeal involvement: A case report. [Article in French]. J Radiol 2004;85(1):51–3. [CrossRef]
[Pubmed]

2.
Karray S, Zlitni M, Fowles JV, et al. Vertebral hydatidosis and paraplegia. J Bone Joint Surg Br 1990;72(1):84–8. [CrossRef]
[Pubmed]
3.
El Andaloussi M, Yousri B, Aboumaarouf M. Vertebral hydatidosis: Three case reports. [Article in French]. Rev Chir Orthop Reparatrice Appar Mot 2001;87(4):392–6.
[Pubmed]
4.
Fahl M, Haddad FS, Huballah M, Kana'an S, Husheimi I, Azizi T. Magnetic resonance imaging in intradural and extradural spinal echinococcosis. Clin Imaging 1994;18(3):179–83. [CrossRef]
[Pubmed]
5.
Tsitouridis I, Dimitriadis AS. CT and MRI in vertebral hydatid disease. Eur Radiol 1997;7(8):1207–10. [CrossRef]
[Pubmed]
6.
Argenson C, Griffet J, Lacour C, Arcamone H, Lovet J, de Peretti F. Vertebral hydatid cyst. Apropos of 2 cases. [Article in French]. Rev Chir Orthop Reparatrice Appar Mot 1989;75(4):267–70.
[Pubmed]
7.
Tekkök IH, Benli K. Primary spinal extradural hydatid disease: Report of a case with magnetic resonance characteristics and pathological correlation. Neurosurgery 1993;33(2):320–3.
[Pubmed]
8.
Hernigou P, Nabih A, Goutallier D. Vertebral hydatidosis. Complications, contribution of modern imaging. [Article in French]. Rev Rhum Mal Osteoartic 1992;59(2):131–5.
[Pubmed]
9.
Chikhaoui N, Adil A, Kadiri R. Radiological aspects of vertebro-medullary hydatid cysts. Apropos of 12 cases. [Article in French]. J Radiol 1993;74(12):621–8.
[Pubmed]
SUPPORTING INFORMATION
Author Contributions
Fabrice Diekouadio - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Steve Semboung - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Beah Boris - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Asaad El Bakkari - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Fatim Zahra Laamrani - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2020 Fabrice Diekouadio et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.