|
Original Article
Correlation of anterio-posterior widths of mandibular condyles with maxillary and mandibular anterior alveolar basal bone heights - A radiological analysis
1 Senior Lecturer, Department of Restorative Dentistry, College of Medicine Lagos State University, Ikeja, Lagos state, Nigeria
2 Lecturer , Department of Restorative Dentistry, College of Medicine Lagos State University, Ikeja, Lagos state, Nigeria
Address correspondence to:
Adolphus Odogun Loto
Lagos State University College of Medicine, Department of Restorative Dentistry, Faculty of Dentistry, Ikeja, Lagos State,
Nigeria
Message to Corresponding Author
Article ID: 100012R02AL2019
Access full text article on other devices

Access PDF of article on other devices


How to cite this article
Loto AO, Adenuga-Taiwo OA. Correlation of anterioposterior widths of mandibular condyles with maxillary and mandibular anterior alveolar basal bone heights - A radiological analysis. Edorium J Radiol 2019;5:100012R02AL2019.ABSTRACT
Aims: To determine correlation between anterioposterior widths of mandibular condyles, maxillary anterior alveolar basal bone height and mandibular anterior alveolar basal bone height.
Methods: Orthopantomograms (OPG) of 250 patients who attended Lagos State University Hospital Dental Centre were reviewed on specific inclusion and exclusion criteria. The anterioposterior widths of mandibular condyles and maxillary anterior alveolar basal bone height, and mandibular anterior alveolar basal bone height were measured using the digital ruler on the OPG. The obtained values were subjected to descriptive statistical analysis using SPSS Version 20. Variations among the measured parameters were tested using students t-test while correlation between maxillary anterior alveolar basal bone height and mandibular anterior alveolar basal bone weight were tested using Pearson correlation coefficient test. Level of confidence interval was set at 95% while significance level was set at p<0.05.
Results: The mean value of anterio-posterior widths of mandibular condyles was higher in males than females and the mean difference was statistically significant. The mean values of maxillary anterior alveolar basal bone height and mandibular anterior alveolar basal bone height were higher in males than females and the mean differences were statistically significant. There was no statistically significant difference between right and left anterio-posterior widths of mandibular condyles in both sexes.
Conclusion: There was a strong positive correlation of anterioposterior widths of mandibular condyles, maxillary anterior alveolar basal bone height and mandibular anterior alveolar basal bone height.
Keywords: Anterio-posterior widths, Mandibular condyles, Mandibular anterior alveolar basal bone height, Maxillary anterior alveolar basal bone height
INTRODUCTION
The mandibular condyles are major components of temporomandibular joints (TMJs); and they have been subjected to various studies with respect to size and shape. Several studies have shown variations in shape and size based on age, sex, utilization, race, and genetics as well as environmental factors [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14]. Differences have also been observed based on facial type, functional load, occlusal force and malocclusion type and between right and left sides [11],[12],[13],[14].
The mandibular condyles act as sites for adjustable growth under functional load. They also perform joint functions. The morphology is typically characterized by a rounded bone projection with an upper biconvex and oval shape in axial plane. Studies have shown that the anteriorposterior width is shorter than the medio-lateral length; and the medio-lateral length is considered approximately twice the anterior-posterior width [2]. It has also been well established by various researchers that the growth and development of the facial bones, including the mandible, have been directly linked to muscular activities of the orofacial muscles, which may function as isolated groups or in a combined and coordinated manner based on their attachments and orientations [11],[12],[13],[14].
The morphology of TMJs have been studied by different methods which include dry human skulls, histology, radiographic examination, magnetic resonance, traditional computed tomography, cone beam computed tomography and panoramic radiograph. Although the panoramic radiograph has its limitations to evaluate the accuracy of condylar morphology, it has been widely utilized in clinical settings.
Studies on the linear and angular measurements of mandible and maxilla have shown wide variations from different ethnic populations all over the world [8],[9],[10]. However, the proportional relationships between the various components of the mandible and maxilla have been employed as diagnostic tools as well as treatment planning resources in the management of orthodontic, prosthodontics and surgical orthognathic patients. Literature is very sparse on the correlation of the size of mandibular condyles with the maxillary and mandibular anterior alveolar basal bone heights. Therefore, the objectives of this study were:
- To determine the anterio-posterior widths of mandibular condyles in a group of Nigerians;
- To determine the existence, if any, of correlation between the anterio-posterior width of mandibular condyles (APWC) and maxillary anterior alveolar basal bone height (MaxAABBH) as well as mandibular anterior alveolar basal bone height (MandAABBH).
MATERIALS AND METHODS
This was a retrospective study based on the radiographic assessment of mandibular condyles with respect to their anterior-posterior widths (APWs) in comparison with mandibular and maxillary anterior alveolar basal bone heights. Two hundred and fifty digital orthopantomograms (OPG) of patients who attended the Dental Centre, Lagos State University Teaching Hospital were reviewed based on the following inclusion criteria:
- Clear and well-defined radiograph showing the definite morphology of the mandibular condyles;
- Radiograph must have good contrast;
- The exposure time of the radiograph must be indicated;
- The magnification factor must be indicated;
- The voltage and current of the machine must be indicated;
- There should be no history of orthodontic treatment, fracture of the mandible; ankylosis of TMJs and Neuromyopathies; and
- The upper and lower dental rows must be complete.
The exclusion criteria included the following:
- Poor and ill-defined radiograph of the mandibular condyles;
- Poor radiographic contrast;
- No indication of the exposure time of the radiograph;
- No indication of the magnification factor;
No indication of the voltage and current of the machine; - History of orthodontic treatment, fracture of the mandible; ankylosis of TMJs and Neuromyopathies; and
- Incomplete upper and lower dental rows.
Out of the 250 digital radiographs that were reviewed, only sixty met the inclusion criteria. The anterior-posterior width of each condyle was measured on the radiograph by drawing two parallel lines that were tangential to the most posterior and most anterior landmarks on the head of the condyle. The values for the left and right condyles were read from the digital ruler on the radiographs. A pair of divider was also used to measure the APWC; and the values were read from the digital ruler on the radiographs (Figure 1).
The alveolar-basal bone heights of the maxilla and mandible were also measured on the panoramic radiographs at the mid-sagittal line as follows:
For the mandibular alveolar basal bone height, the distance between the crest of the alveolar bone and the inferior border of the mandible (in the midline) was measured as the anterior alveolar basal bone height (MandAABBH) using a divider; and the value was read on the vertical digital ruler on the radiograph. Similar procedure was carried out on the maxillary alveolar-basal bone height (MaxAABBH) using the alveolar crest in the midline and the base of the anterior nasal spine as the landmarks (Figure 1).
The author was first trained prior to the actual measurements of the selected radiographs. This was done by measuring ten radiographs by the author in the first instance; and these radiographs were re-measured one week after the first measurements were carried out. The values obtained from the two separate set of measurements were compared; and there were no significant variations.
Three measurements were carried out on each condyle, MandAABBH, and MaxAABBH. The mean of the three measurements was found for each condyle, MandAABBH, and MaxAABBH.
The obtained values were analyzed using descriptive statistics such as frequency, mean and standard deviation. Correlation of anterio-posterior width (APW) of the mandibular condyles with the maxillary and mandibular alveolar basal bones’ heights was determined using Pearson’s correlation test; and the significant level was set at p≤0.05 using confidence interval level of 95%.

RESULTS
The results of this study were presented in tabular form as shown in (Table 1),(Table 2),(Table 3),(Table 4),(Table 5),(Table 6).
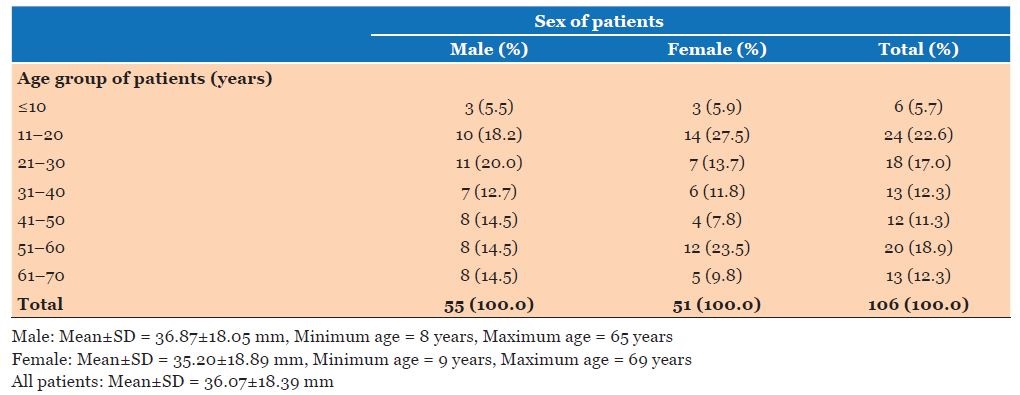
The mean age for male and female was 36.87±18.05 mm and 35.20±18.89 mm respectively while the combined (male and female) mean age was 36.07±18.89 mm (Table 1). There was no statistically significant difference in the mean age between male and female with p-value of 0.613 (Table 2).
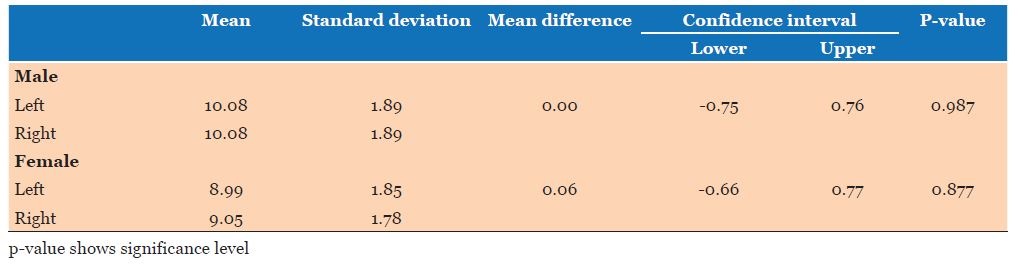
The mean values for anterior-posterior widths of left and right condyles in males were 10.08±1.89 mm and 10.08±1.89 mm respectively while females’ left and right condyles exhibited mean values of 8.99±1.85 mm and 9.05±1.78 mm respectively with a combined mean value of 9.55±1.88 mm. There was no statistically significant difference between the left and right condyles in both sexes; and the p-values for male and female were 0.987 and 0.877 respectively (Table 3).
The mean values for mandibular and maxillary alveolar basal bones’ heights for males were 40.09±7.53 mm and 20.10±3.73 mm respectively while that of female was 37.01±7.33 mm and 18.47±3.63 mm respectively (Table 4). There was statistically significant difference between mean mandibular alveolar basal bone height and mean maxillary alveolar basal bone height in both sexes (p ≤0.000) (Table 4).
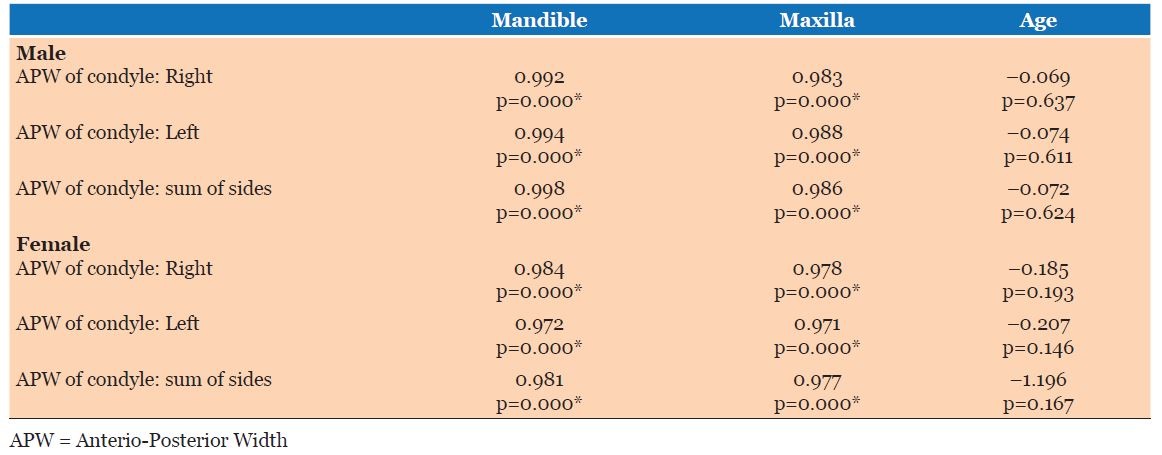
Correlation of APWC with mandibular alveolar basal bone heights (MandAABBH) in males, using Pearson’s correlation test, showed very strong positive correlation coefficients of 0.992, 0.994 and 0.998 between right APWC and MandAABBH, left APWC and MandAABBH and combined right and left APWC and MandAABBH respectively (Table 5). It was also observed that very strong positive correlation coefficients of 0.983, 0.988 and 0.986 were recorded in males between right APWC and MaxAABBH, left APWC and MaxAABBH and sum of left and right APWC and MaxAABBH respectively. However, moderate negative correlation coefficients of -0.069, -0.074 and -0.072 were observed in males between right APWC and age, left APWC and age; and sum of left and right APWC and age respectively (Table 5).
Concerning the female subjects, in this study, it was observed that very strong positive correlation coefficients of 0.984, 0.972 and 0.981 occurred between right APWC and MandAABBH, left APWC and MandAABBH and sum of left and right APWC and MandAABBH respectively (Table 5). It was also noted that strong positive correlation coefficients of 0.978, 0.971 and 0.977 occurred between right APWC and MaxAABBH, left APWC and MaxAABBH; and sum of left and right APWC and MaxAABBH respectively (Table 5). However, moderate negative correlation coefficients of -0.185, -0.207 and -1.196 were also observed in female subjects between right APWC and age, left APWC and age, and sum of left and right APWC and age respectively (Table 5).
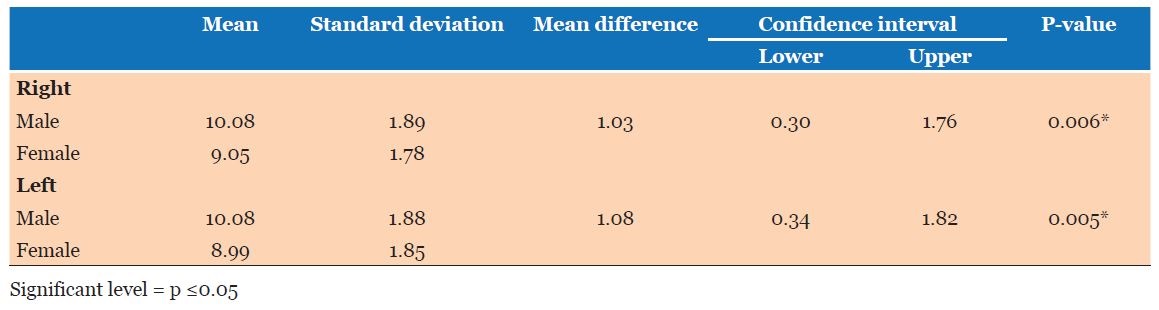
A comparison between the combined mean values of left and right APWCs in male and female subjects revealed that males had higher mean values for right and left (right 10.08±1.89 mm and left 10.08±1.89 mm) compared to females’ mean values of APWC (right 9.05±1.78 mm and left 8.99±1.85 mm). The differences in the mean values for both left and right condyles in respect of both sexes, were statistically significant with p-value of 0.006 for right condyle and p-value of 0.005 for left condyle (Table 6).
The mean ratios of MandAABBH and MaxAABBH to APWC were approximately 4:1 and 2:1 respectively. (Table 7).



DISCUSSION
The establishment of specific correlations among the various TMJ anthropometric measurements as well as other facial measurements has been a veritable tool in the diagnosis, treatment and evaluation of TMJ and occlusal disorders. In this study, it was observed that there was no statistical significant difference between mean values of the right and left APWC in both sexes. However, there was statistical significant difference in mean values of APWC between male and female (Right p-value = 0.006) and (Left p-value = 0.005) (Table 6). This finding was in agreement with the observations of Celik et al [9], Rodrigues et al. [15] and Lascala et al. [16] in their respective studies; and this could be due to a larger bone development in males compared to females.
The mean values of APWC in male (10.08 mm) and female (9.02 mm), in this study, were comparable with the radiographic finding of the study conducted by Hilgers et al. [17] in which they compared the accuracy of different imaging methods in the assessment of temporomandibular joint elements; and found that the mean value obtained from lateral cephalographs of the studied subjects was 11.08 mm. However, the study of Hilgers et al. [17] showed statistically significant difference in the mean values between anatomical truth (8.8 mm) (actual measurement of APWC) and panoramically determined APWC (11.08 mm). The study of Hilgers et al. [17] also showed high degree of accuracy when they compared the mean value of APWC using CBCT with mean value of actual measurement of APWC (anatomical truth); and they obtained a ratio of 1:1. However, the study of Matsumoto and Bolognese [18] did show lower mean values of APWC and mediolateral width (MLW) of condyle for men (8.42 mm and 18.98 mm) respectively compared to females (8.25 mm and 18.92 mm) respectively. Nonetheless, there were no statistically significant differences in these findings. The study of Matsumoto and Bolognese [18] was based on dry skulls with mandibles; and this could account for the lower mean values, obtained in their study, owing to a reduction in the dimensions of the condyles as a result of loss of water content of the mandible.
The mean values of MandAABBH were greater than the mean values of MaxAABBH in both sexes; and there were statistical significant differences between the mean values of MaxAABBH and MandAABBH in both the sexes (p = 0.000). This finding was in consonance with the finding of Beckman et al. [19]. The mandible provides attachment sites for the muscles of mastication and muscles of facial expression; and it is the only mobile bone in the orofacial region characterized by high degree of muscular activities. These high muscular activities could account for the greater development of its alveolar basal bone height compared to that of maxilla.
In this study, the mean values of MaxAABBH and MandAABBH were higher in males (20.01 ±3.73 mm and 40.09±7.53 mm) compared to females (18.47±3.63 mm and 37.01±7.33 mm). However, these differences were not statistically significant (MandAABBH p-value=0.094 and MaxAABBH p-value=0.072). This finding was in agreement with the studies of Celik et al. [9] and Beckman et al. [19]. The higher mean values of MaxAABBH and MandAABBH in males compared to females could be attributed to a larger bone development in males owing to greater muscular and hormonal activities.
This study also showed very strong positive correlations between APWC and MaxAABBH as well as APWC and MandAABBH. This observation could be attributed to the contributory role of condyle in the growth and development of alveolar bone. Schneider and Meyer [20],[21] and Cimasoni and Becks [12], in experimental studies, released occlusion of crowns of the posterior teeth in rats so as to separate the upper and lower teeth; and they observed accelerated growth rates of alveolar crest and inter-radicular bones. This was explained based on the facts that there are two physiological processes, which create separation of upper and lower dentitions condylar growth and attrition. The occurrence of these processes is associated with an increased growth rate of alveolar bone for the purpose of re-establishment of normal occlusion. It should be noted that the anterior face height is dependent upon the condylar growth, the height of the ramus and the posterior alveolar basal bone height [12],[20],[21]. Therefore, it could be inferred that the mandibular and maxillary anterior alveolar basal bone heights, which constitute a major portion of the anterior face height, have a direct association with condylar growth centre which is a major growing site of the length and height of the mandible.
It was noted that this study did not show any direct correlation between APWC and increasing age. This could imply that APWC is established in the early years of development of the mandible; and it does vary a little with increasing age [22]. Therefore, there is no direct proportionality between APWC and increasing age of male and female subjects in this study. This finding corroborates the finding of the study of Valladres [22] in which APWC and medio-lateral width of condyle (MLWC) were examined by CBCT radiography in subjects aged 3–20 years. It was found that no direct association exists between APWC and increasing age. Furthermore, the mean ratios of MandAABBH to APWC and MaxAABBH to APWC for males and females, in this study, were (3.977: 1 and 1.994:1) and (4.103:1 and 2.017:1) respectively (Table 7). In other words APWC for males or females multiplied by approximately two will be equivalent to MaxAABBH while APWC multiplied by approximately four will be equivalent to MandAABBH. If APWC multiplied by two is equivalent to mediolateral width of condyle (MLWC) as previously inferred in this discussion and observed in the previous studies conducted by Celik et al. [9] and Valladres et al. [22], then, the MaxAABBH and MandAABBH for males and females can also be determined from MLWC. However, there is need for further studies in this regard.
LIMITATIONS
The limitations of this study include:
- The anterio-posterior dimension of each mandibular condyle was based on radiographic measurement which had been shown to exhibit significant variation between actual measurement and panoramic measurement; and
- Panoramic radiograph has its limitation to evaluate the accuracy of condylar morphology compared with newer radiographic methods.
CONCLUSION
The anterio-posterior width of mandibular condyles can be utilized to determine the normal heights of maxillary alveolar-basal bone height and mandibular anterior alveolar basal bone height with a view to assessing bone loss, bone augmentation, height of denture bases, crown height, implant length and anterior face height in edentulous patients.
REFERENCES
1.
Ricketts RM. Variations of the temporomandibular joint as revealed by cephalometric laminagraphy. Am J Orthod 1950;36(12):877–98.
[Pubmed]

2.
Solberg WK, Hansson TL, Nordström B. The temporomandibular joint in young adults at autopsy: A morphologic classification and evaluation. J Oral Rehabil 1985;12(4):303–21. [CrossRef]
[Pubmed]
3.
Lindblom G. Status of temporomandibular joint in aged persons. Int Dent J 1964;14:389–94.
4.
Goldman SM, Taylor R. Retrospective radiographic evaluation of 100 temporomandibular joint patients. J Prosthet Dent 1985;53(4):566–9.
[Pubmed]
5.
Gianelly AA, Ruben MP, Risinger R. Effect of experimentally altered occlusal vertical dimension on temporomandibular articulation. J Prosthet Dent 1970;(6)24:629–35. [CrossRef]
[Pubmed]
6.
Oberg T, Carlsson GE, Fajers CM. The temporomandibular joint. A morphologic study on a human autopsy material. Acta Odontol Scand 1971;29(3):349–84.
[Pubmed]
7.
Ebner KA, Otis LL, Zakhary R, Danforth RA. Axial temporomandibular joint morphology: A correlative study of radiographic and gross anatomic findings. Oral Surg Oral Med Oral Pathol 1990:69(2):247–52.
[Pubmed]
8.
Yale SH, Allison BD, Hauptfuehrer JD. An epidemiological assessment of mandibular condyle morphology. Oral Surg Oral Med Oral Pathol 1966;21(2):169–77.
[Pubmed]
9.
Celik MH, Sargon MF, Celik HH. Gross anatomic and scanning electron microscopic studies on the mandibular condyles of the human cadavers. Okajimas Folia Anat Jpn 1998;75(2–3):87–95.
[Pubmed]
10.
Hegde S, Praveen BN, Shetty SR. Morphological and radiological variations of mandibular condyles in health and diseases: A systematic review. Dentistry 2013;3(1):154. [CrossRef]
11.
Burke G, Major P, Glover K, Prasad N. Correlations between condylar characteristics and facial morphology in Class II preadolescent patients. Am J Orthod Dentofacial Orthop 1998;114(3):328–36.
[Pubmed]
12.
Cimasoni G, Becks H. Growth study of the rat mandible as related to function. Angle Ortho 1963;33:27–34.
13.
Cimasoni G. Histopathology of the temporomandibular joint following bilateral extractions of molars in the rat. Oral Surg Oral Med Oral Pathol 1963;16:613–21.
[Pubmed]
14.
Chen J, Sorensen KP, Gupta T, Kilts T, Young M, Wadhwa S. Altered functional loading causes differential effects in the subchondral bone and condylar cartilage in the temporomandibular joint from young mice. Osteoarthritis Cartilage 2009;17(3):354–61. [CrossRef]
[Pubmed]
15.
Rodrigues AF, Fraga MR, Vitral RW. Computed tomography evaluation of the temporomandibular joint in Class I malocclusion patients: Condylar symmetry and condyle-fossa relationship. Am J Orthod Dentofacial Orthop 2009;136(2):192–8. [CrossRef]
[Pubmed]
16.
Lascala CA, Panella J, Marques MM. Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCT-NewTom). Dentomaxillofac Radiol 2004;33(5):291–4. [CrossRef]
[Pubmed]
17.
Hilgers ML, Scarfe WC, Scheetz JP, Farman AG. Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofacial Orthop 2005;128(6):803–11. [CrossRef]
[Pubmed]
18.
Matsumoto MA, Bolognese AM. Bone morphology of the temporomandibular joint and its relation to dental occlusion. Braz Dent J 1995;6(2):115–22.
[Pubmed]
19.
Beckmann SH, Kuitert RB, Prahl-Andersen B, Segner D, The RP, Tuinzing DB. Alveolar and skeletal dimensions associated with lower face height. Am J Orthod Dentofacial Orthop 1998;113(5):498–506.
[Pubmed]
20.
Schneider BJ, Meyer J. Experimental studies on the interrelations of condylar growth and alveolar bone formation. Angle Orthod 1965;35:187–99.
[Pubmed]
21.
Meyer J, Schneider BJ, Das AK. Experimental studies on the interrelations of condylar growth and alveolar bone formation. II. Effects of growth hormone. Angle Orthod 1967;37(4):309–19.
[Pubmed]
22.
Neto JV, Estrela C, Bueno MR, Guedes OA, Porto OCL, Pécora JD. Mandibular condyle dimensional changes in subjects from 3 to 20 years of age using Cone-Beam Computed Tomography: A preliminary study. Dental Press J Orthod 2010;15(5):172–81. [CrossRef]
SUPPORTING INFORMATION
Author Contributions
Adolphus Odogun Loto - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Olugbenga Adetokunbo Adenuga-T - Conception of the work, Design of the work, Acquisition of data, Analysis of data, Drafting the work, Revising the work critically for important intellectual content, Final approval of the version to be published, Agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Guaranter of SubmissionThe corresponding author is the guarantor of submission.
Source of SupportNone
Consent StatementWritten informed consent was obtained from the patient for publication of this article.
Data AvailabilityAll relevant data are within the paper and its Supporting Information files.
Conflict of InterestAuthors declare no conflict of interest.
Copyright© 2019 Adolphus Odogun Loto et al. This article is distributed under the terms of Creative Commons Attribution License which permits unrestricted use, distribution and reproduction in any medium provided the original author(s) and original publisher are properly credited. Please see the copyright policy on the journal website for more information.